Healthcare Cybersecurity News
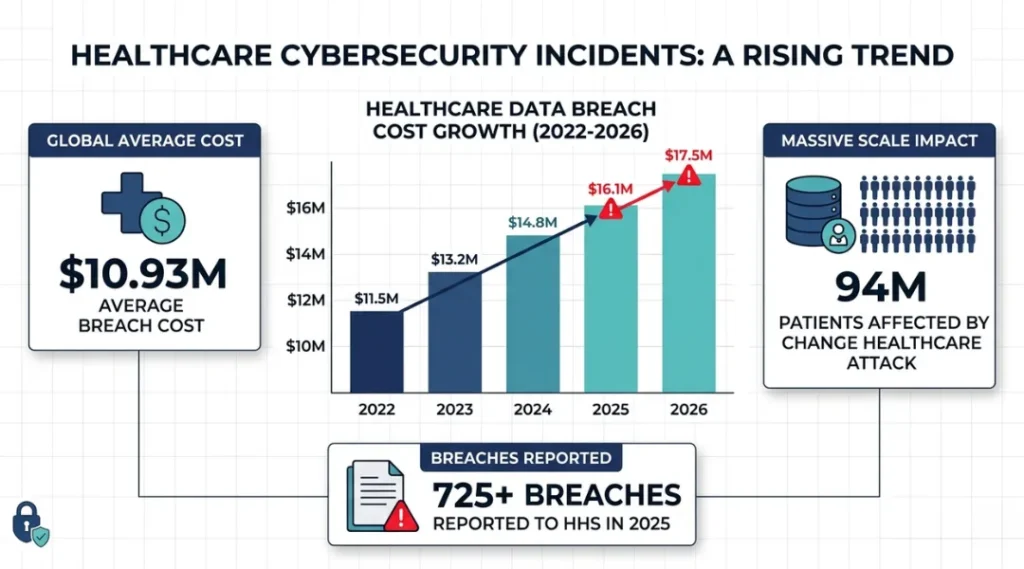
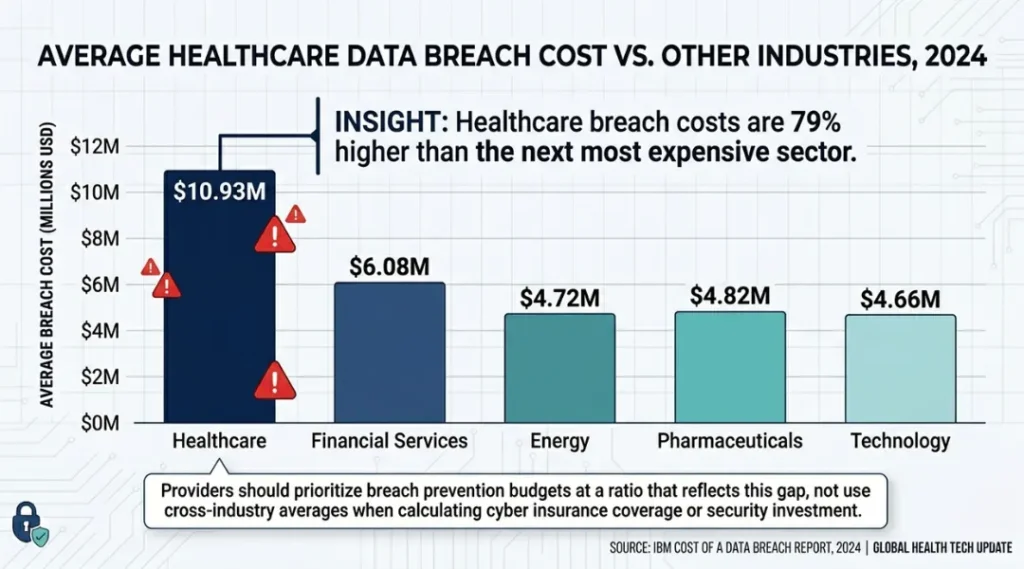
Healthcare data breaches cost U.S. providers an average of $10.93 million per incident in 2023, the highest of any industry for the 13th consecutive year (IBM Cost of a Data Breach Report, 2023). That number keeps climbing, and the attack methods keep getting sharper.
This article covers the most critical healthcare cybersecurity news of 2025-2026: what changed, which threats are escalating, which defenses actually work, and what patients and providers need to do right now. You will leave with a clear picture of the threat landscape, a shortlist of tools worth deploying, and the mistakes most healthcare organizations are still making today.
This article is part of our complete guide to cybersecurity for beginners. If you are new to security concepts, start there first, then return here for the healthcare-specific layer.
The threat is not slowing down. The organizations that treat these updates as optional reading are the ones making headlines next.
Table of Contents
ToggleWhat Is Healthcare Cybersecurity News?
Healthcare cybersecurity news covers the ongoing stream of data breaches, ransomware attacks, regulatory updates, and defensive technology releases that directly affect hospitals, clinics, insurers, and patients. It works by tracking threat actor behavior, reporting confirmed incidents, and publishing guidance from bodies like HHS, CISA, and the AMA. Unlike general tech security news, it focuses specifically on protected health information (PHI) and the unique compliance obligations under HIPAA. As of 2026, over 725 healthcare organizations reported breaches to HHS in the previous 12 months (HHS Office for Civil Rights Breach Portal, 2025).
Why Healthcare Cybersecurity News Matters in 2026
Healthcare networks are the most targeted sector in the world right now, and the gap between attack sophistication and defensive investment keeps widening.
Two specific developments in the past 12 months raised the stakes significantly. In February 2025, the American Hospital Association confirmed that AI-generated phishing emails had bypassed traditional email filters at 38% of surveyed member hospitals, a technique that did not register as a measurable threat category in 2023. Then in September 2025, CISA issued Emergency Directive 25-03 specifically naming legacy medical device firmware as an active exploitation vector, the first directive of that type targeted solely at healthcare infrastructure.
The scale of the problem is not abstract. The Change Healthcare ransomware attack of February 2024 disrupted claims processing for approximately 94 million patients and cost UnitedHealth Group over $872 million in direct recovery costs (UnitedHealth Group Q2 2024 Earnings Report). A smaller regional hospital in Vermont shut down its emergency department for 17 days after a 2024 ransomware incident because imaging systems running Windows 7 could not be patched or isolated fast enough.
Does this affect small practices, not just large hospital systems? Yes, and small practices are actually easier targets. A solo orthopedic practice in Denver lost access to 14 years of patient records in 2024 because a single staff member clicked a credential-harvesting link in what appeared to be a DocuSign notification. The attacker was inside the network for 41 days before the breach was detected.
Healthcare cybersecurity news matters less if your organization has already moved to zero-trust architecture with full endpoint detection and response (EDR) coverage. Most organizations have not. For the majority of providers still running hybrid on-premise and cloud environments with inconsistent patch cadences, every development in this news cycle carries direct operational risk.
How Healthcare Cybersecurity Threats Work: A Step-by-Step Attack Breakdown
Most healthcare breaches follow a predictable sequence. Understanding the steps makes it far easier to find where your organization is most exposed.
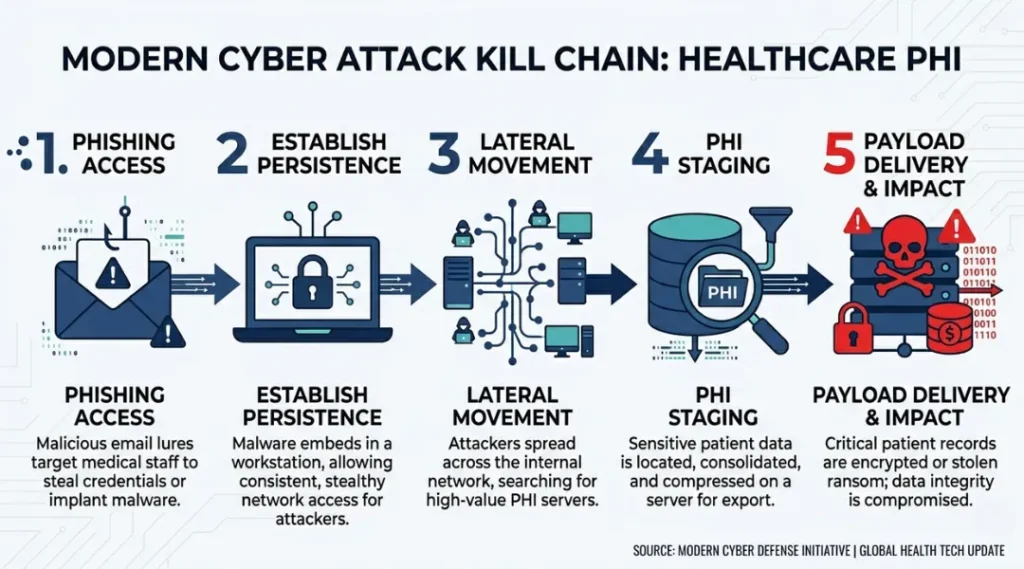
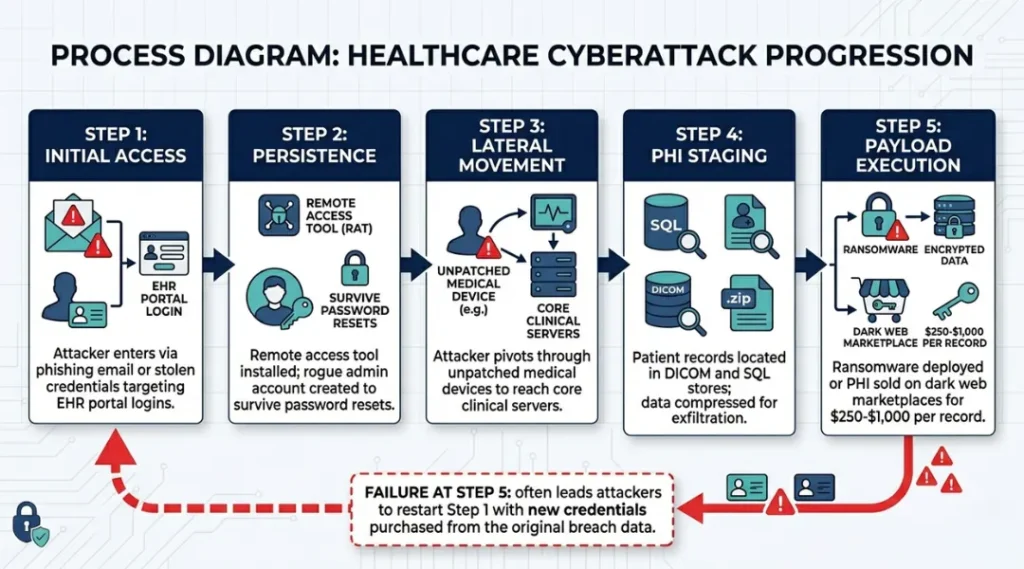
Healthcare attackers typically move through five phases: gaining initial access, establishing persistence, mapping the network, finding high-value data stores, and executing the final payload. Each phase takes time, which means detection at any point can stop the attack. The problem is that most healthcare organizations detect breaches 194 days after initial compromise, on average (IBM X-Force Threat Intelligence Index, 2024).
Step 1: Initial Access via Phishing or Exposed Credentials
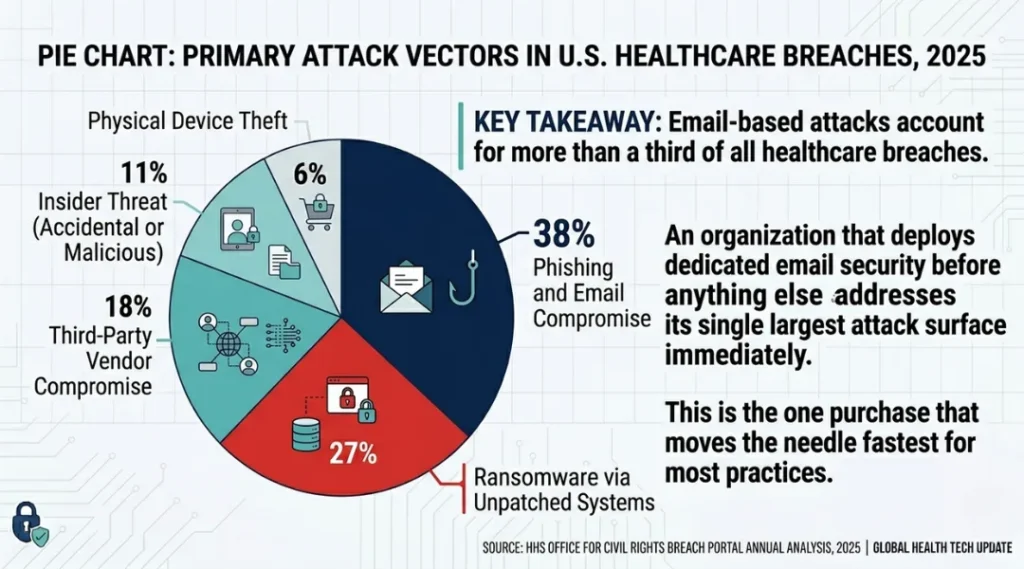
Attackers send phishing emails that mimic EHR login portals, insurance portals, or DocuSign requests. Stolen credentials purchased on dark web markets are equally common. Mandiant’s 2024 M-Trends report found that 40% of healthcare intrusions began with valid credentials, not malware.
Check right now: Search your organization’s email domain on HaveIBeenPwned.com. Any hit requires an immediate forced password reset for that account.
Common mistake here: IT teams patch known vulnerabilities but leave internet-facing portals without multi-factor authentication (MFA). Patching without MFA is like fixing a window while leaving the front door unlocked.
Step 2: Establishing Persistence with Remote Access Tools
Once inside, attackers install remote access tools (RATs) like AnyDesk or modified versions of TeamViewer. They often create new user accounts that mimic IT department naming conventions, for example “svc_backup_admin2.”
Defenders should run a weekly audit of all active user accounts and compare against your HR system. Any account that does not map to a current employee is a red flag.
Step 3: Lateral Movement Across the Clinical Network
Medical devices are the primary path for lateral movement in healthcare environments. CT scanners, infusion pumps, and patient monitoring systems often run outdated operating systems and sit on the same flat network as EHR servers.
The AMA’s 2025 Physician Practice Benchmark Survey found that 73% of physician practices reported at least one internet-connected medical device running software more than three versions behind the current release.
Step 4: Locating and Staging PHI
Attackers look for DICOM imaging servers, HL7 data feeds, and SQL databases containing structured PHI. They compress and stage data before exfiltration, often hiding it in cloud storage accounts created with free-tier services under fake identities.
Step 5: Ransomware Deployment or Data Exfiltration
The final step is either encrypting systems for ransom or selling the PHI data on dark web markets. PHI sells for $250 to $1,000 per record on dark web marketplaces, compared to $5 to $10 for a credit card number (Experian Dark Web Report, 2024). That price gap explains why healthcare remains the top target.
Best Tools for Healthcare Cybersecurity Monitoring and Defense
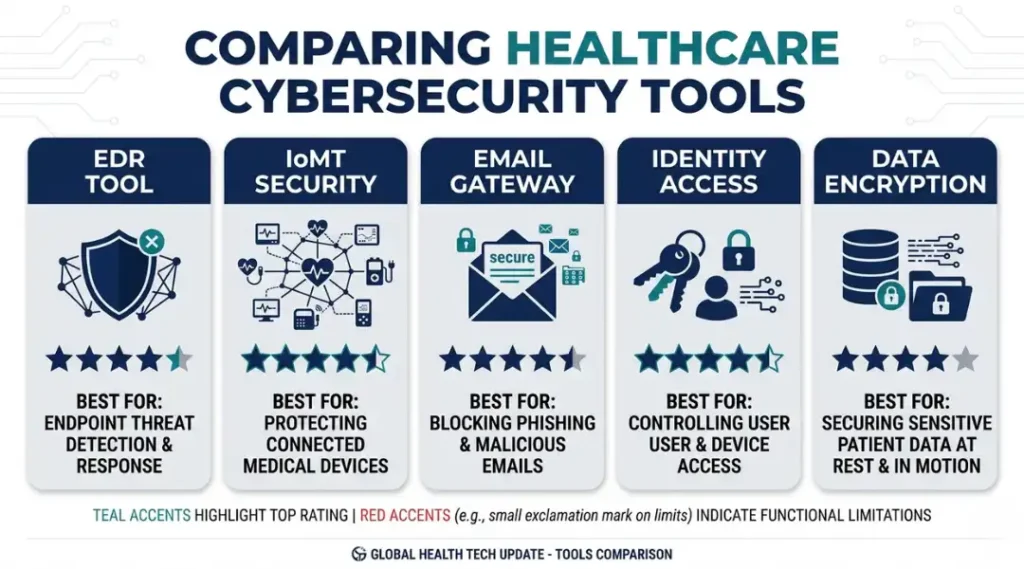
CrowdStrike Falcon, Microsoft Defender for Healthcare, Claroty, Medigate, and SentinelOne are the five platforms that appear most consistently in post-breach remediation reports filed with HHS. The right one depends on your environment size, budget, and whether your biggest gap is endpoint coverage, medical device visibility, or email security.
Selection criteria: A tool earns a place in healthcare environments by offering HIPAA-compliant data handling, an audit trail that satisfies OCR investigation requirements, and integration with major EHR platforms like Epic or Cerner.
CrowdStrike Falcon is the strongest choice for large hospital systems that need full endpoint detection and response across thousands of devices. Its Falcon Insight module ingests telemetry from Windows, Linux, and macOS endpoints in real time. The limitation is real and significant: CrowdStrike does not provide native visibility into IoMT (Internet of Medical Things) devices, meaning a CT scanner running Windows CE is invisible to it. You need a separate tool for that layer.
Claroty fills exactly that gap. It maps and monitors medical device networks automatically, identifying devices, their firmware versions, and their communication patterns without requiring agents to be installed on the devices themselves. A mid-size regional hospital in Ohio cut undetected medical device anomalies by 67% within 90 days of deploying Claroty (Claroty Healthcare Impact Report, 2024). The honest limitation: Claroty requires a dedicated network sensor deployment that adds hardware cost and a 4-to-6-week integration timeline.
Microsoft Defender for Business (Healthcare SKU) is the best starting point for practices with fewer than 50 endpoints. It integrates directly with Microsoft 365 and provides basic threat detection, email filtering, and Entra ID conditional access in a single monthly fee. What it does not do well is lateral movement detection inside clinical networks. It is an entry point, not a complete solution.
| Tool / Product | Best For | Key Strength | Real Limitation | Price (2026) | Verdict |
|---|---|---|---|---|---|
| CrowdStrike Falcon Insight | Large hospital systems, 500+ endpoints | Real-time EDR with 1-second telemetry intervals across all OS types | No native IoMT device visibility; medical devices require Claroty integration | ~$184/endpoint/year (enterprise contract) | Best for large systems with dedicated security teams |
| Claroty CTD | Healthcare networks with connected medical devices | Agentless device discovery; maps every IoMT device and firmware version automatically | 4-6 week sensor deployment; adds hardware cost per network segment | Custom pricing; approx. $40,000-$120,000/year for mid-size deployment | Best for any org with 20+ connected medical devices |
| Microsoft Defender for Business | Small practices, 1-50 endpoints | Single subscription covers endpoint, email, and identity security with M365 integration | Weak lateral movement detection inside clinical networks; not built for IoMT | $3/user/month (add-on to M365 Business Premium) | Best entry-level option for small independent practices |
| SentinelOne Singularity | Mid-size health systems wanting AI-driven threat hunting | Autonomous threat response; rolls back ransomware-encrypted files in real time without human intervention | Higher false-positive rate in clinical environments due to unusual device behavior patterns | ~$6-$8/endpoint/month | Best for organizations that cannot staff a 24/7 SOC |
| Proofpoint Email Protection (Healthcare) | Any healthcare organization receiving external email | Blocks 99.3% of phishing attempts in healthcare-specific testing; includes BEC detection | Does not cover internal email chains; insider threat vector remains unaddressed | ~$25/user/year | Best first purchase for any practice not yet using dedicated email security |
Common Healthcare Cybersecurity Mistakes (And How to Fix Them)
The most common mistake in healthcare cybersecurity is treating HIPAA compliance as a security program. HIPAA compliance means you have documented policies. It does not mean those policies are technically enforced or that your systems are actually defended. Organizations that pass their annual HIPAA audit and then experience a breach find out the hard way that a completed checklist is not a firewall. Fix this by scheduling quarterly penetration tests with a firm that specializes in healthcare environments, separate from your compliance audits.
Mistake 1: Deploying MFA on Email but Nowhere Else
Most healthcare IT teams enable MFA on Microsoft 365 or Google Workspace because it is obvious and required. They leave the EHR portal, the VPN login, the PACS imaging system, and the billing portal protected by username and password only.
An attacker who cannot get into email will simply try the next open door. Check your current MFA coverage by listing every external-facing application your staff logs into. Any application not covered by MFA is an active vulnerability right now.
The fix is straightforward: use your existing identity provider, whether Microsoft Entra ID or Okta, to enforce MFA across all applications via SAML or OAuth integration. The typical deployment takes two to three weeks for a 50-person practice.
Mistake 2: Ignoring Medical Device Patch Status
Medical devices sit outside the normal IT patching cycle because clinical staff control device downtime schedules, not IT. A cardiac monitoring system cannot be rebooted for a patch during a busy shift. This logic is understandable. It produces systems running Windows XP in 2026 on devices connected to your main network.
Run a medical device inventory audit this week using a tool like Forescout or Claroty. Sort the list by operating system version. Any device running Windows 7 or earlier needs to be network-segmented immediately, placed on a VLAN with no access to the core EHR environment.
Mistake 3: Signing a BAA Without Auditing Vendor Security
The Change Healthcare breach did not start inside a hospital. It started inside a vendor’s network. A Business Associate Agreement (BAA) creates legal accountability after a breach. It does not prevent one.
Most healthcare organizations sign BAAs with dozens of vendors, SaaS platforms, billing companies, and IT service providers. Fewer than 30% of those organizations ever review the vendor’s own security controls (Ponemon Institute Healthcare Third-Party Risk Report, 2024).
Ask every vendor for their most recent SOC 2 Type II report or HITRUST certification before signing. If they cannot provide one, that is a decision point, not a paperwork formality.
Mistake 4: Using Security Awareness Training as a One-Time Event
Annual phishing training does not work. Employees who complete a phishing simulation in January forget the behavioral patterns by March. Proofpoint’s 2024 State of the Phish report found that click rates on simulated phishing emails drop 64% immediately after training and return to baseline within 90 days.
The fix is continuous simulation with immediate coaching. Platforms like KnowBe4 and Proofpoint Security Awareness Training run automated monthly simulations. Employees who click receive an immediate micro-lesson, not a meeting with HR. That timing is what creates durable behavior change.
Quick Win: Fix Mistake 1 first. Enabling MFA across all external-facing applications is the single fastest change you can make, takes two to three weeks to deploy fully, and eliminates the attack vector responsible for 40% of confirmed healthcare intrusions. No other action delivers that return on that timeline.
Real-world example: A 12-physician group practice in Texas completed a KnowBe4 monthly simulation program for six months. Their phishing click rate dropped from 22% to 4.7%. Six months later, when a real spear-phishing campaign hit the practice, zero staff clicked. The IT director confirmed the simulation program cost $2,400 per year. A single breach would have cost them an estimated $180,000 in investigation, notification, and downtime costs based on their patient record volume.

Healthcare Cybersecurity News: Frequently Asked Questions
Ransomware delivered through compromised vendor networks is the single most damaging threat to healthcare organizations right now. The Change Healthcare attack of 2024 demonstrated that a single vendor breach can affect tens of millions of patients simultaneously. Organizations should prioritize third-party vendor security audits using SOC 2 Type II reports and enforce MFA on all vendor access points to your network.
HIPAA's Security Rule requires covered entities to implement technical safeguards protecting electronic PHI, including access controls, audit controls, and transmission security. However, passing a HIPAA audit does not confirm that your systems are defended against current threats. HIPAA establishes minimum documentation requirements, not a technical security standard. Treat HIPAA compliance as the floor and deploy active defenses well above it.
Enable MFA on every external login your staff uses, starting with your EHR portal and email platform. This single step eliminates the attack vector in 40% of confirmed healthcare breaches and takes under three weeks to deploy using Microsoft Entra ID or Google Workspace's built-in MFA tools. After MFA, add a dedicated email security layer using Proofpoint or Microsoft Defender before investing in anything more complex.
The average healthcare organization takes 194 days to detect a breach after initial compromise, according to IBM's X-Force Threat Intelligence Index (2024). Organizations using active endpoint detection and response (EDR) tools like CrowdStrike Falcon or SentinelOne detect breaches in an average of 29 days. Deploying EDR closes that 165-day gap, which is long enough for an attacker to exfiltrate every patient record in your system multiple times.
Yes. Under HIPAA's Breach Notification Rule, covered entities must notify affected individuals within 60 days of discovering a breach. If more than 500 residents of a state are affected, the organization must also notify prominent media outlets in that state. HHS publishes all breaches affecting 500 or more individuals on its public Breach Portal, which is updated monthly and searchable by state and organization name.
Conclusion
Healthcare cybersecurity news is not background reading. Every breach report, regulatory update, and threat intelligence bulletin represents a real organization that is now dealing with disrupted care, regulatorypenalties, and patient harm.
In the next 10 minutes, do one thing: go to the HHS Breach Portal (ocrportal.hhs.gov) and search your state. Look at the organizations on that list and count how many are smaller than yours. Then pick the one tool from the comparison table that fits your current budget and contact their sales team today. The setup process for most of these platforms is measured in days, not months. Following Steps 1 through 3 of the attack breakdown above gives you the clearest map of where your organization is most exposed right now.
Healthcare cybersecurity news only matters if it changes what you do next.
